Ethnic inequalities in loneliness in Britain during the COVID-19 pandemic: Evidence for Equality National Survey (EVENS)
Zeng-Hui Ma, Patricia Irizar, Aradhna Kaushal
Posted by Giaoa Robinson
Score:
Importance – 4
Strength of Evidence – 4
Clarity – 4
PEER REVIEW:
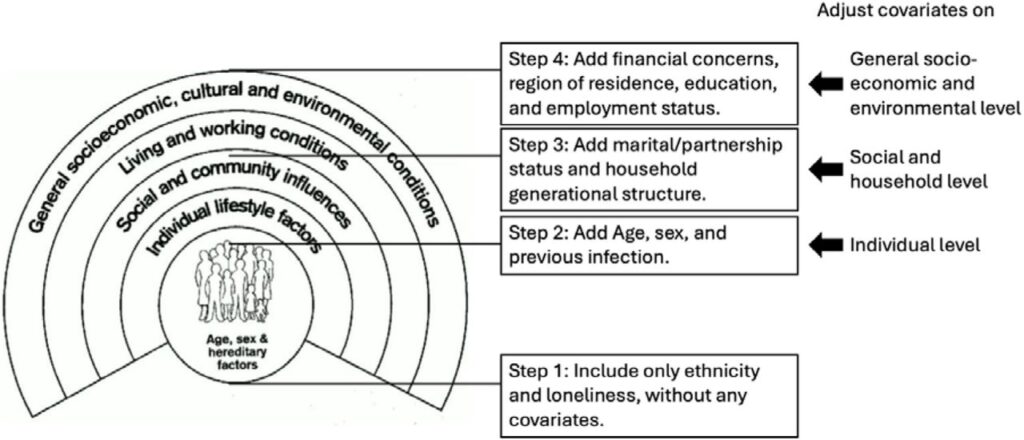
This exploratory cross-sectional study by Ma et al. (2025) examines ethnic inequalities in loneliness across 21 disaggregated ethnic groups in Britian during the COVID-19 pandemic, using data from the Evidence for Equality National Survey (EVENS). Weighted logistic regression models assess this relationship in disaggregated (n=21) and aggregated(n=6) ethnic groups, both unadjusted and adjusted for several sociodemographic covariates. Findings of higher odds of loneliness among most ethnic minority groups in the disaggregated model are consistent with previous studies that observed higher rates of COVID-19 related infections, hospitalization, ICU admission, and death compared to the White population in Britain, inferring that aggregation can have a masking effect. While adjusting for age and sex explained disparities in some groups, additional factors likely underlie observed differences in others. Generally, this paper seeks to build on previous literature and well-established methodology to assess an understudied, long-term health outcome of the COVID-19 pandemic. It leverages preexisting EVENS data to conduct comprehensive analyses, including comparative aggregated analyses and exploratory disaggregated analyses to offer new insights into ethnic disparities of loneliness and include historically underrepresented groups. It uses several sampling methods, including snowballing, open link survey, survey panels, and community-based interviews, to recruit a relatively large sample (n=14,215)and does achieve a very high response rate over the course of the study period (February to November 2021). However, the number of disaggregated ethnic groups of interest (n=21)and the amount of weighting to reduce selection bias and coverage bias required for analyses suggest the need for a larger, more representative sample to increase internal validity and confidence. A more nuanced and compelling set of analyses should also explicitly discuss other major determinants or proxies for loneliness, specifically measures of pre-existing loneliness (i.e., before the pandemic), substance use, and mental health conditions and diagnoses, such as anxiety or depression. Moreover, considering other social covariates like and immigrant status or an assessment of community/social involvement could afford additional insights into self-reported and cultural perceptions of loneliness. Finally, the authors are encouraged to share their suggestions of culturally tailored interventions, as well as how they might build on their findings to design and implement such a study. Very minor comment, but the authors should provide justification for why the sample age does not extend beyond 75 years, as many people beyond this age reside in assisted living facilities and were severely impacted by lockdown measures.
Preprint Links